
Cardiac insufficiency
Cardiac insufficiency (medically known as ‘heart failure’) means that the strength of the heart muscle is not sufficient to pump enough blood to the various organs.
Cardiac insufficiency can have many different causes. Typical symptoms include tiredness, reduced performance, shortness of breath, lack of appetite and swollen legs.
Cardiac insufficiency
Cardiac insufficiency (medically known as ‘heart failure’) means that the strength of the heart muscle is not sufficient to pump enough blood to the various organs.
Cardiac insufficiency can have many different causes. Typical symptoms include tiredness, reduced performance, shortness of breath, lack of appetite and swollen legs.
The symptoms of cardiac insufficiency can be very unspecific, such as fatigue or decreasing performance. Cardiac arrhythmias also occur more frequently. Depending on which of the two sides of the heart is primarily affected, other symptoms may also occur:
Left side of heart weak:
- Shortness of breath under stress, when speaking or even at rest
- Discomfort when lying flat (upper body elevation necessary)
- Dizziness
Right side of heart weak:
- Decreased appetite with pressure/feeling of fullness in the right upper abdomen
- Swelling of the legs/lower legs/ankles
- Declining performance
It can therefore be the result of valvular heart disease, blocked coronary arteries, arrhythmia, high blood pressure or a combination of such conditions.
However, it can also develop directly as a heart muscle disease. It can be triggered by congenital heart disease or diseases of other organs. However, external factors such as infections, radiation and drug treatments (especially chemotherapy) can also lead to cardiac insufficiency.
Since a variety of problems can ultimately lead to cardiac insufficiency, many different, but not always all, of the clarifications listed below are often necessary:
- Assessment of symptoms and medical history
- Physical examination incl. blood pressure measurement
- Resting ECG
- Exercise ECG
- Blood tests on various organ systems (heart, liver, kidneys, infections…)
- Cardiac ultrasound examination
- Heart MRI
- CT of the coronary vessels
- Cardiac catheter examinations
- Heart muscle biopsy
We distinguish between general and specific therapies.
General therapies:
- Optimization of risk factors:
- Nutritional optimization
- Weight reduction (with/without medication)
- Stop smoking
- Physical activity
- Blood pressure and diabetes control
- Treatment of iron deficiency
- drug treatment:
- diuretic medication
- Medication against cardiac arrhythmia
- specific cardiac insufficiency medication
- Inhibitors of the renin-angiotensin-aldosterone system (ACE inhibitors, sartans, sacubitril-valsartan, aldosterone receptor antagonists)
- SGLT2 inhibitors
Specific therapies:
- Treatment of the underlying problem (e.g. replacement of a narrow or leaking heart valve, treatment of blocked coronary arteries, elimination of arrhythmia, etc., see the ‘Therapy’ section for the respective heart disease)
- Cardiac resynchronization therapy (see below)
- Implantation of a defibrillator (see below)
- LVAD – left ventricular assist devices
- Heart transplantation
The symptoms of cardiac insufficiency can be very unspecific, such as fatigue or decreasing performance. Cardiac arrhythmias also occur more frequently. Depending on which of the two sides of the heart is primarily affected, other symptoms may also occur:
Left side of heart weak:
- Shortness of breath under stress, when speaking or even at rest
- Discomfort when lying flat (upper body elevation necessary)
- Dizziness
Right side of heart weak:
- Decreased appetite with pressure/feeling of fullness in the right upper abdomen
- Swelling of the legs/lower legs/ankles
- Declining performance
Cardiac insufficiency is the end stage of various heart diseases that could not be treated in time or effectively.
It can therefore be the result of valvular heart disease, blocked coronary arteries, arrhythmia, high blood pressure or a combination of such conditions.
However, it can also develop directly as a heart muscle disease. It can be triggered by congenital heart disease or diseases of other organs. However, external factors such as infections, radiation and drug treatments (especially chemotherapy) can also lead to cardiac insufficiency.
Since a variety of problems can ultimately lead to cardiac insufficiency, many different, but not always all, of the clarifications listed below are often necessary:
- Assessment of symptoms and medical history
- Physical examination incl. blood pressure measurement
- Resting ECG
- Exercise ECG
- Blood tests on various organ systems (heart, liver, kidneys, infections…)
- Cardiac ultrasound examination
- Heart MRI
- CT of the coronary vessels
- Cardiac catheter examinations
- Heart muscle biopsy
We distinguish between general and specific therapies.
General therapies:
- Optimization of risk factors:
- Nutritional optimization
- Weight reduction (with/without medication)
- Stop smoking
- Physical activity
- Blood pressure and diabetes control
- Treatment of iron deficiency
- drug treatment:
- diuretic medication
- Medication against cardiac arrhythmia
- specific cardiac insufficiency medication
- Inhibitors of the renin-angiotensin-aldosterone system (ACE inhibitors, sartans, sacubitril-valsartan, aldosterone receptor antagonists)
- SGLT2 inhibitors
Specific therapies:
- Treatment of the underlying problem (e.g. replacement of a narrow or leaking heart valve, treatment of blocked coronary arteries, elimination of arrhythmia, etc., see the ‘Therapy’ section for the respective heart disease)
- Cardiac resynchronization therapy (see below)
- Implantation of a defibrillator (see below)
- LVAD – left ventricular assist devices
- Heart transplantation
Specific therapies for cardiac insufficiency
Dyssynchrony is both a cause and a consequence of cardiac insufficiency. This means that the left and right ventricles are no longer stimulated to beat at the same time, but at different times. This dyssynchrony means that the pumping action is no longer effective and it itself exacerbates the cardiac insufficiency (vicious circle).
Improve synchrony
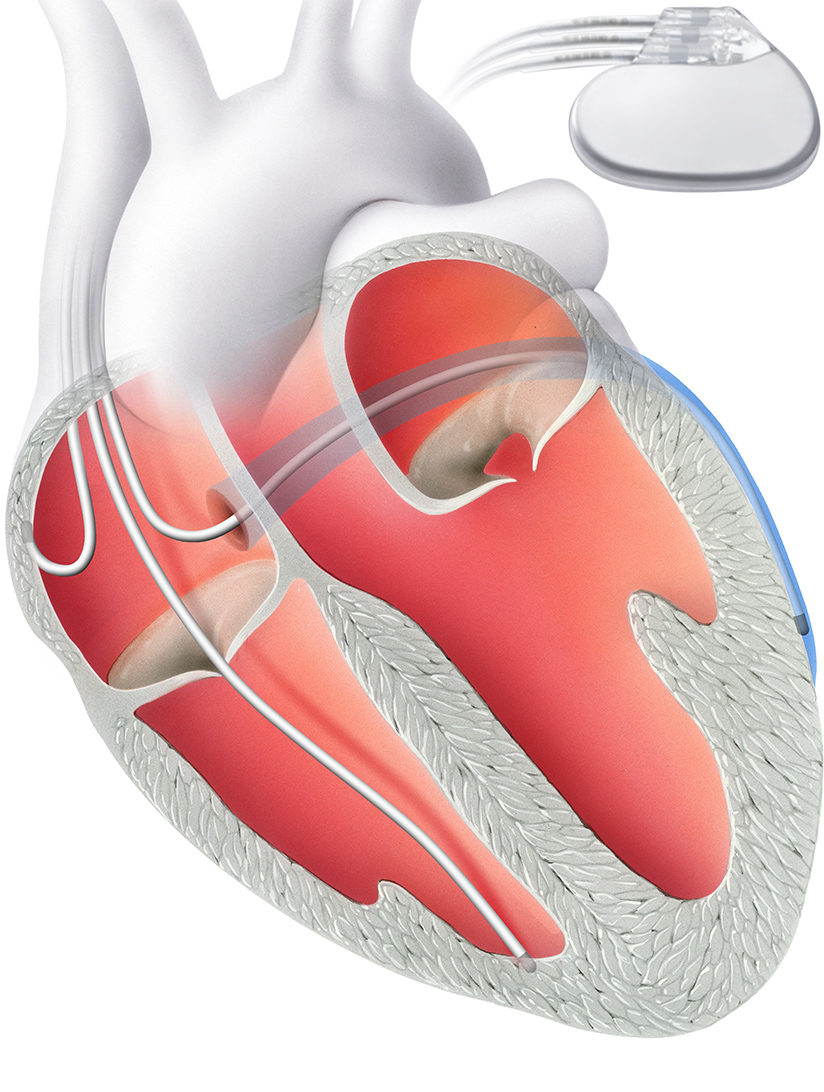
Cardiac resynchronization therapy (CRT) corrects this problem. It aims to improve the synchrony of the left and right ventricles. A biventricular pacemaker, i.e. one that stimulates both ventricles, is implanted for this purpose.
This does not have two electrodes like a conventional pacemaker, but three. The additional electrode is inserted into a coronary vein in front of the left ventricle. Alternatively, it can be inserted via a thoracoscopic approach, a minimal incision in the chest.
Thanks to this third electrode, it is possible to stimulate both ventricles at the same time. A hospital stay of two to three days is required for the procedure.
If there is a high risk of life-threatening cardiac arrhythmia, it may be necessary to implant an internal shock device (ICD). The ICD is implanted under local anesthesia in a similar way to a pacemaker.
The defibrillator continuously monitors the heart rhythm and detects a rapid and life-threatening heart rhythm. In this case, it can restore the normal heart rhythm by overstimulation or by delivering an electric shock.
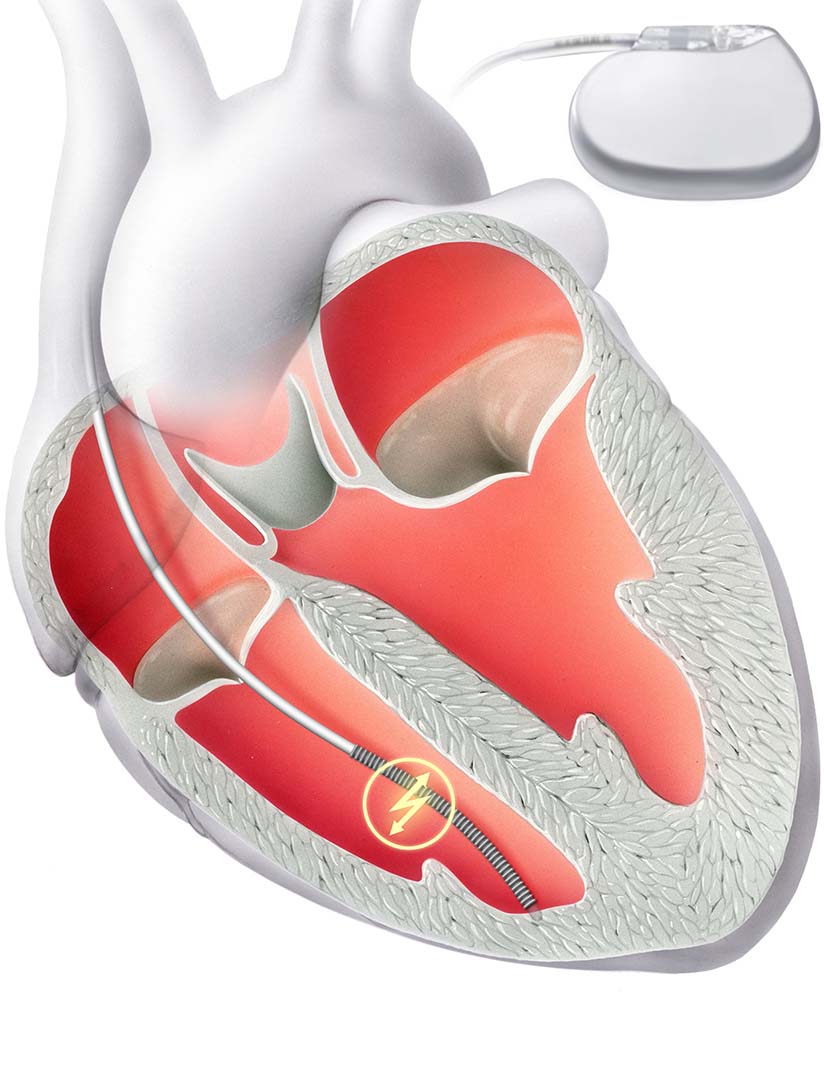
Similar to a pacemaker, the defibrillator consists of two components: Firstly, an electrode that is anchored in the right ventricle via the vein. The second is a device with a battery, which is implanted under the skin.
In standard ICD therapy, an electrode is implanted directly into the heart. It is part of a defibrillator that can normalize the rhythm if the heartbeat is too fast.
The subcutaneous ICD (S-ICD) has been available as an alternative for almost 10 years. With this form of therapy, the heart and blood vessels remain unaffected: an electrode is not implanted directly into the heart, but above the sternum directly under the skin (“subcutaneously”). This significantly reduces the risk of electrode complications and complications during possible electrode removal. However, the risk of so-called “inadequate shock delivery” (“misfires”) is slightly higher than with standard ICDs with electrodes in the heart.
Dyssynchrony is both a cause and a consequence of cardiac insufficiency. This means that the left and right ventricles are no longer stimulated to beat at the same time, but at different times. This dyssynchrony means that the pumping action is no longer effective and it itself exacerbates the cardiac insufficiency (vicious circle).
Improve synchrony
Cardiac resynchronization therapy (CRT) corrects this problem. It aims to improve the synchrony of the left and right ventricles. A biventricular pacemaker, i.e. one that stimulates both ventricles, is implanted for this purpose.
This does not have two electrodes like a conventional pacemaker, but three. The additional electrode is inserted into a coronary vein in front of the left ventricle. Alternatively, it can be inserted via a thoracoscopic approach, a minimal incision in the chest.
Thanks to this third electrode, it is possible to stimulate both ventricles at the same time. A hospital stay of two to three days is required for the procedure.
If there is a high risk of life-threatening cardiac arrhythmia, it may be necessary to implant an internal shock device (ICD). The ICD is implanted under local anesthesia in a similar way to a pacemaker.
The defibrillator continuously monitors the heart rhythm and detects a rapid and life-threatening heart rhythm. In this case, it can restore the normal heart rhythm by overstimulation or by delivering an electric shock.
Similar to a pacemaker, the defibrillator consists of two components: Firstly, an electrode that is anchored in the right ventricle via the vein. The second is a device with a battery, which is implanted under the skin.
In standard ICD therapy, an electrode is implanted directly into the heart. It is part of a defibrillator that can normalize the rhythm if the heartbeat is too fast.
The subcutaneous ICD (S-ICD) has been available as an alternative for almost 10 years. With this form of therapy, the heart and blood vessels remain unaffected: an electrode is not implanted directly into the heart, but above the sternum directly under the skin (“subcutaneously”). This significantly reduces the risk of electrode complications and complications during possible electrode removal. However, the risk of so-called “inadequate shock delivery” (“misfires”) is slightly higher than with standard ICDs with electrodes in the heart.
Further information


Our specialists for cardiac insufficiency
Cardiac insufficiency

Prof. Dr. med.
Prof. Dr. med.
Georg Noll
Georg Noll
Cardiology | Prevention
Cardiology | Prevention
DE – EN – FR – IT
DE – EN – FR – IT
ICD

Prof. Dr. med.
Prof. Dr. med.
Jürg Grünenfelder
Jürg Grünenfelder
Cardiac surgery
Cardiac surgery
DE – EN – IT – FR
DE – EN – IT – FR
CRT & ICD


